Questions on history and general examination
History taking
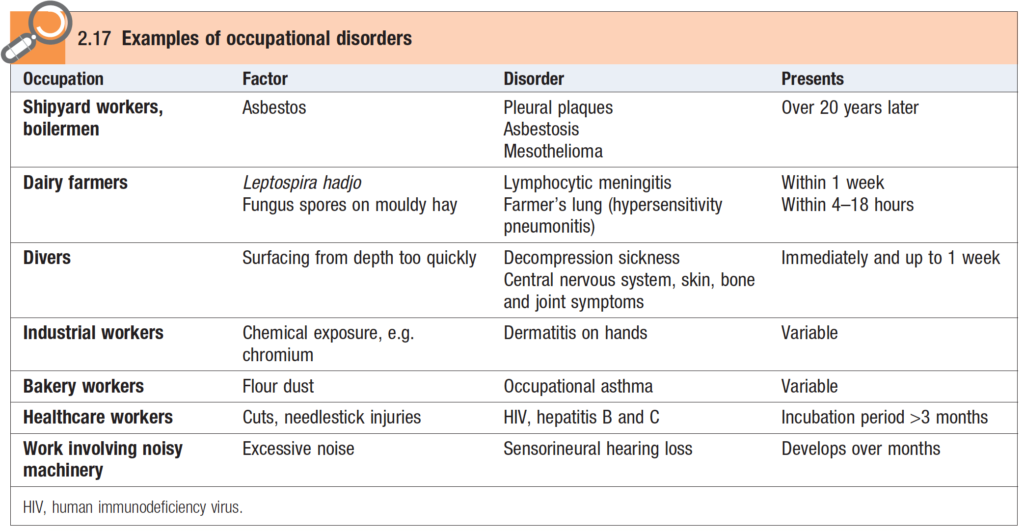
- Mention clinical importance of taking occupational history.
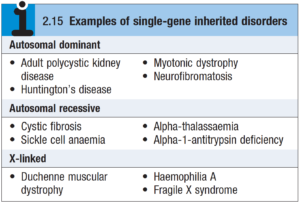
- Mention clinical importance of taking family history.
- Mention the diseases you can encounter in a smoker
General examination
- Q
Rimikri
SOLVES
History taking
Mention clinical importance of taking occupational history.
* Macleod’s Clinical Examination, 13th Edition
Mention clinical importance of taking family history.
Many illnesses are associated with a positive family history. Such as –
- Cardiovascular and cerebrovascular: Hypertension, IHD, CVD
- Respiratory system: Atopic asthma, emphysema, TB
- Gastrointestinal system: Irritable bowel syndrome (IBS), inflammatory bowel disease (IBD), peptic ulcer disease, polyps, colorectal cancer
- Genitourinary system: Prostate carcinoma
- Breast: Breast cancer
* Macleod’s Clinical Examination, 13th Edition; Oxford Handbook of Clinical Medicine, 9th Edition
Mention the diseases you can encounter in a smoker
The dangers of cigarette smoking
- General
- Lung cancer
- Chronic obstructive pulmonary disease (COPD)
- Carcinoma of the oesophagus
- Ischaemic heart disease
- Peripheral vascular disease
- Bladder cancer
- An increase in abnormal spermatozoa
- Memory problems
- Maternal smoking
- A decrease in birth weight of the infant
- An increase in fetal and neonatal mortality
- An increase in asthma
- Passive smoking
- Risk of asthma, pneumonia and bronchitis in infants of smoking parents
- An increase in cough and breathlessness in smokers and non-smokers with COPD and asthma
- An increase in cancer risk
* Kumar and Clark’s Clinical Medicine, 9th Edition
Examination of face, tongue
How examination of face helps in clinical diagnosis of diseases?
| Disorder | Appearance |
| Acromegaly | Coarsening with enlarged features, e.g. nose, lips, orbital ridges and jaw (prognathism) |
| Hypothyroidism | Pale, puffy skin with loss of lateral third of eyebrows |
| Hyperthyroidism | Startled appearance with lid retraction |
| Cushing’s disease | ‘Moon face’, plethoric complexion and buffalo hump over lower cervical—upper thoracic spine |
| Parkinsonism | Expressionless facies and drooling |
| Myasthenia gravis | Expressionless facies with bilateral ptosis |
| Myotonia dystrophica | Frontal baldness and bilateral ptosis |
| Superior vena caval obstruction | Plethoric, oedematous face and neck, chemosis of conjunctivae, prominent veins and venules |
| Malar flush | Dusky redness of cheeks seen in low cardiac output, e.g. mitral stenosis; also seen in myxoedema |
| Systemic lupus erythematosus | Rash over nose and cheeks — ‘butterfly rash’ |
| Progressive systemic sclerosis | Taut skin around mouth with ‘beaking’ of nose |
* Macleod’s Clinical Diagnosis, 1st Edition
What diagnoses are possible by looking at the tongue?
- Dry or moist
- Dry: Dehydration, mouth breathing xerostomia (in Sjogren syndrome), anticholinergic drug therapy.
- Moist: Sialorrhoea in postencephalitic Parkinsonism, local mouth infection, gastroesophageal reflux disease (GERD), heavy metal poisoning.
- Colour
- Pale: Anaemia.
- Yellow: Jaundice (mainly in undersurface of tongue).
- Bluish: Central cyanosis, methaemoglobinaemia, sulphaemoglobinaemia (mainly involves the sides of the tongue), blue coloured food material.
- Bluish red: Polycythaemia.
- Black tongue (lingua nigra): Ingestion of bismuth, liquorice, charcoal, etc., Addison disease (pigmented).
- Brownish: CKD.
- Magenta coloured: Riboflavin (vitamin B2) deficiency.
- Raw beefy tongue (red, swollen and painful): Vitamin B12 deficiency, niacin deficiency (pellagra).
- White patches over tongue: Candidiasis, leukoplakia, chronic superficial glossitis.
- Black hairy tongue: Smoking, fungal infection, tetracycline, penicillins.
- White or greyish coating or”furred tongue’: Smoking, chronic debilitating disease.
- White and red strawberry tongue: Scarlet fever.
- Geographical tongue (there are irregular red and white patches on the tongue. These lesions look like a geographic map. Slowly changing red rings and lines that occur on the surface of the tongue). It has no clinical significance, but, can be a sign of riboflavin deficiency.
- Scrotal tongue (deep horizontal fissure): No clinical significance.
- Mushroom-like tongue (sore tongue with white slough): Corrosive poisoning.
- Blotting paper-like pallor with black pigmentation in the margin: Hook worm infestation.
- Angry looking tongue (central coating with red tip and margins): Enteric fever.
- Glossitis or bald tongue (total loss or atrophy of papillae, smooth tongue): Vitamin B12 deficiency, iron-deficiency anaemia, coeliac disease, pellagra, tropical sprue.
- Mass or ulcers
- Ulcers: Aphthous, malignant, tuberculous, snail track ulcer in secondary syphilis, denture, Crohn disease.
- Bite mark: Convulsion.
- Growth in tongue: Squamous cell carcinoma.
- Hairy leukoplakia (painless white corrugated lesion on sides): Found in AIDS due to EBV infection.
- Papilloma (viral wart)
- Median rhomboid glossitis (lozenge shaped area with loss of papillae and fissuring in the midline of the tongue, anterior to the foramen caecum). It is a congenital anomaly.
- Cysts in the floor of the mouth: Ranula, sublingual dermoid cyst.
- Size and shape
- Macroglossia: Found in Down syndrome, acromegaly, cretinism, myxoedema, primary amyloidosis, mucopolysaccharidosis (e. g., Flurler syndrome), lymphangioma, tumour infiltration.
- Microglossia (atrophy or hemiatrophy): Found in bulbar and pseudobulbar palsy, lower motor neuron (LMN) lesion of Xllth cranial nerve.
- Tongue-tie (ankyloglossia).
- Acute swelling: Infection, angioneurotic oedema.
- Neurological disease
- Flaccid wasted tongue with fasciculation: Bulbar palsy.
- Spastic tongue without fasciculation: Pseudobulbar palsy.
- Jack in the box sign: Rheumatic chorea.
- Tremor: Aruciety neurosis, thyrotoxicosis, chronic alcoholism, Parkinsonism.
- Deviation of the tongue: Deviated to the opposite side is due to upper motor lesion of the 12th cranial nerve. Deviated to the same side is due to lower motor lesion of the 12th nerve.
- Loss of taste sensation: Anterior 2/3rd by facial nerve, posterior 1/3rd by glossopharyngeal nerve. (Site of taste sensation –sweet at the tip, sour at the margin, bitter at the back and salty at any part of the tongue).
- Fasciculation: Bulbar palsy, LMN palsy of Xllth cranial nerve.
- Trombone tongue: Rapid forward and backward movement of the tongue, found in general paresis of insane (GPI).
- Chewing tongue: Found in athetosis
* Short Cases in Clinical Medicine, ABM Abdullah
Examination of hands
What diagnoses are possible by examining the hands?
- Warm and sweaty hands: Hyperthyroidism
- Cold and sweaty hands: Anxiety
- Cold and dry hand: Peripheral vascular disease
- Large, fleshy and sweaty hand: Acromegaly
- Dry hands with coarse skin: Hypothyroidism
- Delayed relaxation of grip: myotonic dystrophy (diagnosed by handshake or asking the patient to close and open the hands)
- Deformities in the hands and fingures: Myotonic dystrophy, rheumatoid arthritis
- Wrist drop: Radial nerve palsy
- Claw hand: Ulnar nerve palsy
- Carpal spasm: Tetany
- Palm
- Palor: Anaemia
- Yellowish: Anaemia
- Palmar erythema: Chronic liver disease
- Single palmar crease (Simian crease): Down syndrome
- Wasting of palmar muscles: Median and ulnar nerve palsies
- Tremor
- Fine tremor: Anxiety, thyrotoxicosis.
- Resting tremor: Parkinson’s disease.
- Flapping tremor: Liver failure, renal failure, respiratory failure
- Bluish discoloration of the fingers: Cyanosis
- Nail and nail beds
- Clubbing: Suppurative lung disease, bronchial carcinoma, interstitial lung disease, congenital
cyanotic heart diseases, liver cirrhosis, inflammatory bowel disease, familial etc. - Brittle and spoon chaped nail (koilonychia): Iron deficiency anaemia
- Leuconychia: CLD, nephrotic syndrome, PEM
- Splinter haemorrhage: Infective endocarditis
- Brown line pigmentatign: Chronic kidney disease
- Mees line: Arsenic poisoning
- Thickening, crumbing and discoloration: Fungal infection (onychomycosis)
- Onycholysis: Psoriasis
- Beau’s line: Fever, cachexia, malnutriotion
- Clubbing: Suppurative lung disease, bronchial carcinoma, interstitial lung disease, congenital
What are the findings in hand in infective endocarditis?
As follows
- Osler nodes (small painful violaceous raised nodule, 0. 5–1. 5 cm, present on the tip of the fingers and toes, also palmar aspect, probably due to development of vasculitis or septic emboli).
- Splinter haemorrhage
- Clubbing
- Janeway lesion (large painless erythematous macule containing bacteria on palm, pulp of the fingers. It may be found in the sole)
- Petechial haemorrhage
- Infarction on the tip of the fingers
*Short Cases in Clinical Medicine, ABM Abdullah
What are the findings in hand in CLD?
As follows
- Palmar erythema
- Dupuytren contracture
- Clubbing
- Leukonychia
- Flapping tremor
- Spider angioma
- Pigmentation
- Jaundice
- Scratch mark
- Xanthoma
- Cyanosis
*Short Cases in Clinical Medicine, ABM Abdullah
Examination of nails
What diagnoses are possible by examining the nail?
Nail abnormality may occur in many local, systemic and dermatological diseases. These are described below.
- Clubbing, koilonychias, leukonychia
- Pale nail: Anemia
- Nail fold infarction: (usually vasculities due to any cause)
- SLE
- Dermatomyositis
- Systemic sclerosis
- Rheumatoid arthritis (RA)
- Polyarteritis nodosa
- Splinter haemorrhage: Linear dark brown, longitudinal flecks, parallel to long axis of nail.
- Trauma (the commonest).
- SBE
- Septicaemia
- Collagen disease (vasculitis) : SLE, RA and polyarteritis nodosa
- Others : Haematological malignancy, severe anaemia, psoriasis. Rarely in trichinosis (usually transverse haemorrhage).
- Half-and-half nail: Proximal part of nail is white-to-pink and distal part is red or brown. Causes are
- CRF (the commonest cause)
- Cirrhosis of liver
- Occasionally, in normal person
- Red half moon occurs in congestive cardiac failure (CCF).
- Nail fold telangiectasia: Causes are
- SLE
- Systemic sclerosis.
- Dermatomyositis
- Mixed connective tissue disease (MCRD).
- Raynaud phenomenon.
- Beau line: Nonpigmented transverse line or grooves in nail due to transient arrest of nail growth. This appears at the same time, on all the nails, a few weeks after an acute illness. Causes are
- Chronic illness (chronic infection, malignancy and collagen disease).
- Prolonged fever.
- Pneumonia
- Coronary artery disease.
- Others : Cachexia, malnutrition, psychiatric illness, use of cytotoxic drugs.
- Onycholysis: Separation of distal nail plate from the nail bed (free edge looks white). Causes are
- Psoriasis (the commonest).
- Fungal infection.
- Thyrotoxicosis (Plummer sign).
- Idiopathic
- Occasionally drugs (tetracycline and psoralen).
- Porphyria
- Trauma or faulty manicure.
- Mee line: Single transverse white band in nail. Causes are
- Chronic arsenic poisoning
- CRF
- Also, after chemotherapy and severe illness.
- Yellow nail: Found in yellow nail syndrome, an inherited disease in which the nails are thick, yellow or pigmented with separation of distal part of nail bed due to hypoplasia of lymphatic system. It is associated with Iymphoedema of legs, bronchiectasis and pleurai effusion.
- Loss of nail (or dystrophy): Causes are
- Severe lichen planus.
- Epidermolysis bullosa.
- Trauma (tooth biting)
- Nail pitting (depression in nail): Causes are
- Psoriasis
- Alopecia areata.
- Atopic eczema (when involves proximal nail bed).
- Pityriasis rosacea.
- Brittle nail (easily broken): Causes are
- Iron-deficiency anaemia.
- Peripheral vascular disease.
- Fungal infection.
- Hypocalcaemia
- Psoriasis
- Injury (nail biting).
- Idiopathic
- Blue nail: Normal white Iunulae become blue, found in Wilson disease due to deposition of copper (normally, half-moon Iunulae at the proximal end of nail is white-blue half moon). Also found in cyanosis and ochronosis.
- Red nail: May be normal finding. Also in polycythaemia, carbon monoxide poisoning (cherry red).
- Brown nail: Usually present in chronic kidney disease (CKD).
- Periungual or subungual fibroma: Suggests tuberous sclerosis (epiloia).
- Fungal nail: Nail has thick, white, green, black, discolouration and crust formation.
- Absent or small, dysplastic nail: Its causes are
- Nail patella syndrome [autosomal dominant (AD), associated with no or hypoplastic patella and glomerulonephritis, abnormalities in eye].
- Others : Congenital, traumatic and vasculitis.
- Nail hyperpigmentation: May occur due to some drugs (such as zidovudine, doxorubicin, bleomycin, cyclophosphamide, fluorouracil, melphalan and nitrosoureas).
- Terry nail: Proximal part is white or pink, but nail tip is red or brown. It is due to decrease in vascularity and an increase in connective tissue within the nail bed. Causes are
- Old age (normally present in elderly).
- Cirrhosis of liver.
- CCF
- Hyperthyroidism
- Malnutrition
- Renal failure.
- Dark nail: May be a normal finding mostly in black people. Sometimes may be due to subungual melanoma.
Remember the following points
- Normal nail growth is 0.1 mm/day; finger nails grow quickly than toe nails.
- Nail plate grows continuously and slowly at the rate of 1 cm every 3 months. Hence, renewal of finger nails takes about 3-6 months, and toe nails that grow more slowly take 1 year.
- Rapid growth of nail plate occurs in psoriasis.
- Nail growth is arrested by acute illness and ischaemia (Beau line).
*Short Cases in Clinical Medicine, ABM Abdullah
Clubbing
What is differential clubbing and cyanosis?
Differential clubbing and cyanosis mean cyanosis and clubbing of toes, not of the fingers.
- Cause is pulmonary hypertension with shunt reversal in patent ductus arteriosus.
Read more about pda at PDA
* Short and Long Cases in Clinical Medicine, HN Sarker Page: 60